
Knee osteoarthritis (OA) is the most common chronic joint condition, especially affecting individuals over the age of 50. It occurs when the cartilage that protects the bones in the knee joint begins to break down, leading to pain, swelling, and difficulty moving the joint. While knee OA typically affects one knee, both knees may sometimes be involved, particularly in advanced stages. OA is a degenerative condition that worsens with age, and without intervention, it can lead to significant disability and reduced quality of life.
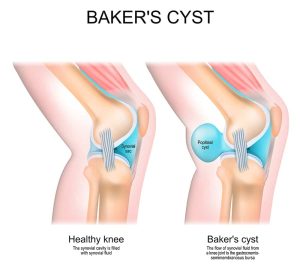
In healthy joints, cartilage acts as a cushion, providing a smooth surface for bones to glide over. However, with osteoarthritis, the cartilage wears down, causing the bones to rub against each other, resulting in pain, stiffness, and swelling in the knee joint.
Knee OA can be classified as primary or secondary, depending on its underlying causes.
Primary Knee OA: This form of OA is related to the natural aging process, where wear and tear cause the cartilage to degrade over time, typically without any specific cause.
Secondary Knee OA: This occurs due to identifiable factors that contribute to the degeneration of cartilage. Common causes include:
Obesity: Excess body weight places additional stress on the knee joints, increasing the risk of OA.
Joint instability: Conditions like joint hypermobility can make the knee more prone to OA.
Misalignment of the knee: Abnormal positioning, such as valgus or varus postures, can lead to uneven wear of the cartilage.
Previous injuries: Knee fractures or other injuries can damage the cartilage, leading to OA over time.
Genetic factors: A family history of OA may increase susceptibility.
Metabolic conditions: Conditions like rickets may also contribute to the development of OA.
Knee osteoarthritis often develops gradually and can cause a range of symptoms, including:
Knee pain that worsens with activity or after prolonged periods of rest.
Knee stiffness and swelling, particularly after long periods of sitting or standing.
A reduced range of motion in the knee, limiting flexibility and mobility.
A grinding or harsh sensation when moving the knee, often due to bone-on-bone contact caused by thinning cartilage.
At York-Med Physiotherapy & Wellness Centre, we specialize in the management of knee osteoarthritis using a holistic, evidence-based approach. Our registered physiotherapists and chiropractors will develop a personalized treatment plan tailored to your unique condition and goals. The following treatments are commonly used:
Manual Therapy: Research shows that manual therapy, when combined with exercise, is highly effective in improving mobility and reducing pain for individuals with knee OA. Our physiotherapists use hands-on techniques to address joint stiffness, improve range of motion, and alleviate discomfort.
Functional Exercise Programs: Our team conducts a comprehensive assessment to identify strength, stability, and mobility deficits. A customized exercise plan is created to address these issues, focusing on strengthening muscles around the knee to improve stability and reduce stress on the joint. Regular exercise evaluations ensure that your program evolves to meet your changing needs. Studies have shown that supervised in-clinic exercises combined with a home exercise program yield better functional outcomes compared to home exercises alone.
Modalities for Pain Relief: We utilize a range of modalities to complement manual therapy and exercises, including:
Acupuncture and dry needling to relieve pain and improve muscle function.
Ultrasound therapy to reduce inflammation and promote healing.
Interferential current therapy to alleviate pain and improve circulation.
Cryotherapy (ice) and heat therapy to manage pain and swelling.
Taping and Bracing: Knee taping and bracing can provide additional support, reduce pain, and improve stability during movement. These techniques are often used in conjunction with exercise to enhance function and prevent further injury.
At York-Med Physiotherapy & Wellness Centre, we are committed to providing top-tier care for knee osteoarthritis. Our approach combines the latest research with personalized treatment strategies to help you manage symptoms, improve joint function, and regain mobility. Whether you’re seeking relief from knee pain or aiming to prevent further deterioration, our expert team is here to support your recovery journey.
© 2020 York-Med Physiotherapy and wellness center | Richmond Hill & Vaughan. All Rights Reserved.
Designed by Magham Agency